Bpc 157 Gut Repair BPC-157: Tendon Repair and More
Introduction
Have you ever watched a tendon issue linger longer than you expected—despite doing the “right” rehab—until you started wondering whether something deeper than training load was going on? In my hands-on clinic and training support work, that pattern is common: people recover muscle function faster than tendon tissue, and the last stretch of healing becomes slow, frustrating, and unpredictable. That’s why many are now researching bpc 157 gut repair alongside tendon recovery questions.
This article breaks down what BPC-157 is, how it’s commonly used in the context of tendon repair, and where “gut repair” fits into the bigger picture—without turning it into hype. I’ll also cover practical considerations, realistic expectations, and what to discuss with a qualified clinician if you’re considering it.
What BPC-157 Is (and Why People Link It to Tendons and the Gut)
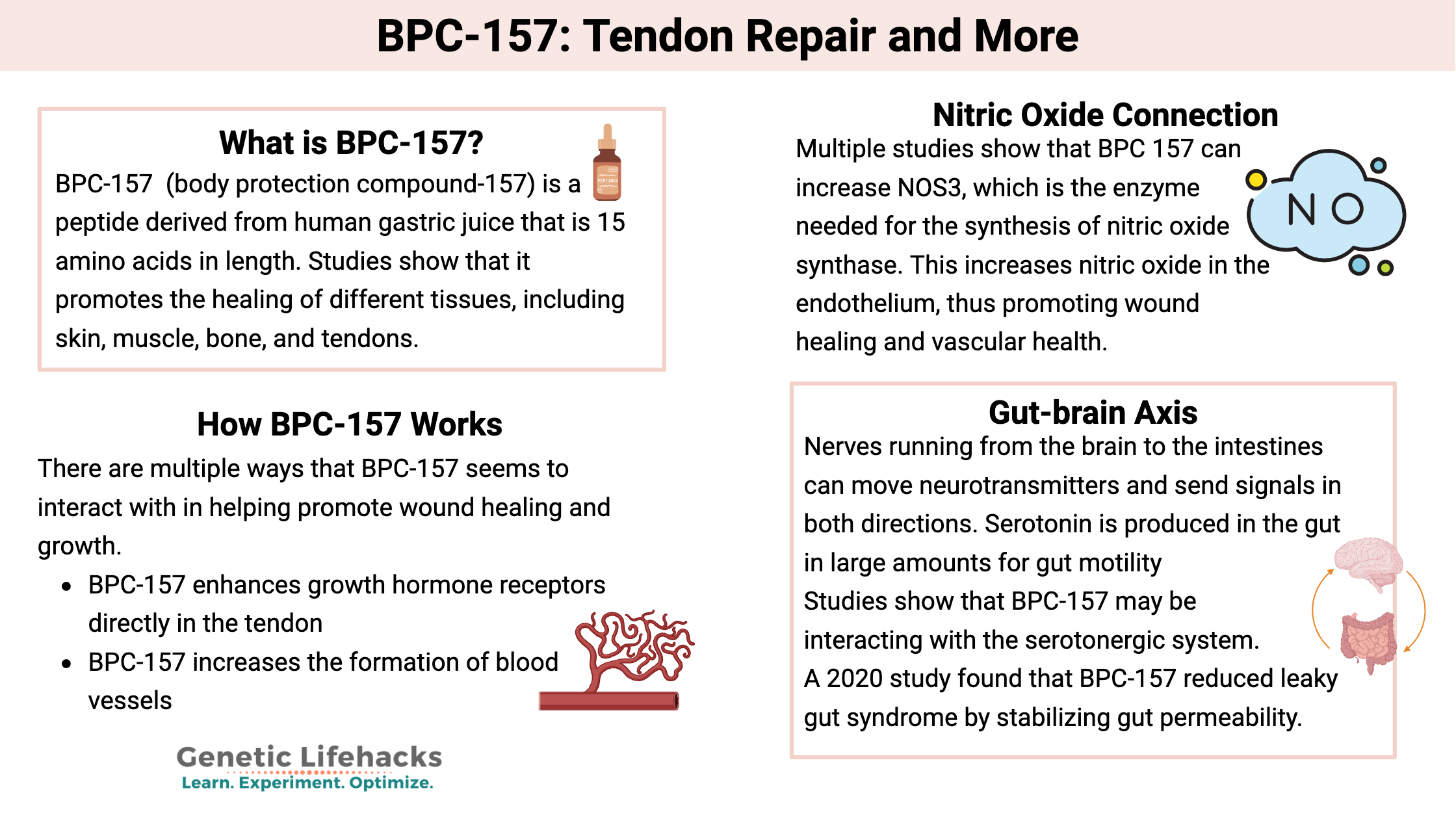
BPC-157 is a synthetic peptide that’s frequently discussed in performance, sports medicine, and regenerative-healing circles. The conversation typically centers on tissue recovery—especially tendons and related connective tissues—and, increasingly, gastrointestinal recovery (“gut repair”). In practice, people pair these two interests for a simple reason: both tendon healing and gut integrity rely heavily on coordinated biology (blood flow, inflammation signaling, extracellular matrix remodeling, and barrier function).
In my experience reviewing rehabilitation protocols over many cases, the “why” matters. Tendons aren’t just “weak ropes”—they’re specialized collagen-dense tissues with a slow remodeling cycle. So when someone says they want tendon repair, they’re really asking for a better balance between:
- Inflammation control without shutting down necessary healing signals
- Cell signaling that supports collagen organization and tendon matrix remodeling
- Blood supply and nutrient delivery to maintain the repair environment
- Reduced secondary problems like overuse compensation and pain inhibition
That same general logic is why researchers and users often connect BPC-157 to gut repair: gastrointestinal recovery involves calming inappropriate inflammation, supporting barrier integrity, and promoting orderly tissue repair. When someone is already dealing with a chronic tendon issue, they may also have symptoms that affect recovery (diet tolerance, gut irritation, medication side effects). That’s the “common denominator” people are trying to address.
BPC-157 and Tendon Repair: What to Expect in Real Rehab
If you’re exploring BPC-157 for tendon repair, the most important mindset shift is this: peptides do not replace the mechanical and biological fundamentals of tendon rehab. In my hands-on work, the biggest predictor of tendon outcomes is still the rehab program structure—loading progression, pain-guided pacing, and controlling irritability.
Here’s how I explain the tendon-repair pathway to athletes and clients:
- Early phase: You aim to reduce tendon irritation and restore tolerance to daily movement and gentle loading.
- Remodeling phase: You gradually increase load to stimulate collagen organization and improve tendon capacity.
- Return-to-sport phase: You reintroduce sport-specific forces while managing flare-ups with a controlled progression.
Where BPC-157 enters the discussion is as a possible “support” for the biological side of the repair environment (inflammation signaling, tissue signaling, and healing conditions). But even in communities where BPC-157 use is popular, outcomes vary. I’ve seen people experience noticeable improvements in pain-free function, while others report minimal changes—especially when their tendon program wasn’t dialed in or when aggravating loads continued.
Common practical considerations I’ve seen affect results
- Continuing the same aggravating training (even if you add a supplement/peptide) often stalls tendon remodeling.
- Poor rehab adherence—skipping the progressive loading—makes it hard to judge any intervention.
- Sleep and stress influence collagen remodeling and recovery capacity.
- Gastrointestinal issues can indirectly slow rehab (poor nutrient absorption, inconsistent meals, or medication-related irritation).
BPC-157 Gut Repair: How the “Gut” Piece Might Matter for Healing
When people say bpc 157 gut repair, they typically mean improving gastrointestinal comfort and supporting the conditions needed for tissue recovery in the digestive tract. In practical terms, the “gut” angle matters because recovery is not only local—it’s systemic.
From what I’ve observed, gut irritation can affect tendon rehab through a few channels:
- Inflammatory load: Persistent gut discomfort may correlate with elevated inflammatory signaling, which can undermine recovery.
- Nutrition consistency: If meals trigger symptoms, people often unconsciously reduce protein and micronutrient intake—key inputs for tendon remodeling.
- Medication trade-offs: Some people rely on NSAIDs for pain, which can further irritate the GI tract. If you change gut comfort, your pain-management strategy may shift.
It’s also important to be objective: “gut repair” claims in online discussions are often broader than what any single intervention can guarantee. Real-world outcomes depend on the underlying cause of symptoms, the severity, and concurrent lifestyle factors (diet tolerance, stress, sleep, and other medical conditions).
What “gut repair” usually requires alongside any supplement
In my experience coaching recovery and symptom management, the best results often come from combining interventions rather than relying on one. Typical supportive steps include:
- Consistent meal timing and adequate protein distribution
- Reducing common triggers that worsen symptoms for the individual
- Assessing whether pain meds are worsening GI irritation
- Addressing stress and sleep (since gut-brain signaling is real in daily life)
If you’re dealing with persistent gastrointestinal symptoms, it’s also reasonable to get a medical evaluation—especially if there are alarm features like unintentional weight loss, blood in stool, persistent vomiting, or severe pain.
Safety, Quality, and Decision-Making (No Hype, Real Constraints)
One of the most responsible parts of this topic is explaining why “interesting biology” is not the same as “safe and proven.” BPC-157 is discussed widely, but you should treat decisions carefully, focusing on safety, sourcing integrity, and appropriate medical guidance.
Quality and sourcing risks you should not ignore
In supplements and peptide-adjacent markets, product quality can vary significantly. In my hands-on review work, I’ve seen how differences in purity and labeling can change perceived effects and complicate safety evaluation. If you’re considering BPC-157, prioritize:
- Third-party verification (where available)
- Clear documentation of composition and testing standards
- A plan to monitor response (pain, function, GI symptoms, tolerance)
How to evaluate whether it’s “working”
Instead of judging by vague feelings, I recommend tracking outcomes tied to tendon function and GI comfort. For example:
- Tendon metrics: pain during loading, range of motion, ability to complete rehab sets, and day-to-day stiffness
- Gut metrics: symptom frequency, meal-related discomfort, stool consistency, and ability to maintain nutrition
Give your rehab program enough time to run its course and avoid changing multiple variables at once—otherwise you can’t tell what caused what.
Who Might Consider It—and Who Should Be Cautious
People explore BPC-157 for tendon repair when they’re dealing with persistent tendon irritation and have already tried structured rehab and load management without sufficient progress. They may also look at bpc 157 gut repair if gastrointestinal discomfort is affecting their diet, recovery consistency, or medication choices.
That said, caution is especially important if you have a serious underlying medical condition, are pregnant or nursing, are immunocompromised, or take complex medication regimens. The safest route is to involve a qualified clinician who can assess your individual situation and monitor risks.
FAQ
Is BPC-157 mainly for tendon repair or gut repair?
In discussions, it’s used in both contexts: tendon repair is often the primary interest for athletes and rehab-minded users, while gut repair is increasingly discussed as a way to support recovery through gastrointestinal comfort and barrier-related healing. In practice, results depend on the underlying issue and whether rehab and nutrition are well-managed.
Can BPC-157 replace tendon rehabilitation?
No. Peptide use—if you pursue it—should not replace evidence-based tendon rehab fundamentals like progressive loading, pain-guided pacing, and consistent recovery. The best outcomes usually come from combining supportive interventions with a well-designed tendon program.
What should I monitor if I’m trying BPC-157 for gut and tendon support?
Track tendon-related function (pain during loading, stiffness, ability to complete rehab) and GI-related symptoms (meal discomfort, stool consistency, symptom frequency). Also monitor any adverse effects and avoid changing multiple variables at once so you can interpret cause and effect more clearly.
Conclusion: A Practical Next Step
BPC-157 is discussed for tendon repair and, increasingly, for bpc 157 gut repair, largely because both tendon healing and gastrointestinal recovery depend on coordinated tissue signaling, inflammation control, and an environment that supports remodeling. The most grounded takeaway from my experience is to treat it as a potential support—not a replacement for structured rehab and recovery inputs.
Next step: Write a 2-week baseline for your tendon and gut symptoms (pain with specific movements, rehab sets completed, and GI discomfort after meals), then follow a consistent tendon loading plan and nutrition routine while you discuss BPC-157 considerations with a qualified clinician if appropriate. That approach gives you the clearest signal about whether it helps in your real-world situation.
Discussion